by Oliver Ruatti
The origins of the myth about fat and the heart
When did the war on fat start? To cholesterol?
In the 1950s, an American physiologist, Ancel Keys, forever changed the way the
world thought of fats.
His theory-that fats in the diet increased cholesterol in the blood and this
caused heart disease-it became the basis of modern nutritional guidelines.
But what was really behind this hypothesis? And how well-founded was it?
From rabbits to humans
Initially, studies on atherosclerosis were based on experiments conducted on the rabbits,
Herbivorous animals that easily developed arterial lesions when fed foods of
animal origin. Keys and other researchers transposed these findings to humans, hypothesizing.
that the dietary cholesterol Was the culprit.
However, as early as the early 1950s, the same human experiments showed.
which increasing cholesterol in the diet did not change cholesterol levels in the
blood.
Keys himself admitted this in 1954: "The cholesterol content of the diet does not have an effect
significant on either blood cholesterol levels or atherosclerosis in humans."
From blaming cholesterol to blaming fat
Having failed to make a direct association between dietary cholesterol and blood cholesterol, Keys changed
target: he decided that the problem was no longer cholesterol, but the total fats.
In 1953 he presented a graph showing an apparent correlation between consumption of
fats and mortality from heart disease In six countries.

calories derived from fat compared to total calories consumed. In a nutshell, the graph
shows: more fat intake=more deaths from heart disease).
But two epidemiologists, Yerushalmy and Hilleboe, they noticed something strange:
data were available for 22 countries, not just six-and, including all of them, the correlation
disappeared.
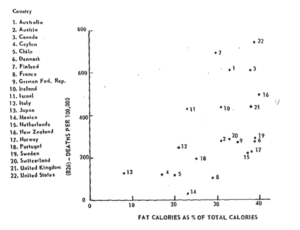
With an increase in deaths from heart disease. For example: In Norway (17) there is a
much higher fat consumption than in Israel (11), but in Norway there are
However, far fewer deaths from heart disease. In Mexico (14) there is a consumption of
fat similar to that of Israel (11), but still in Israel the number of deaths from
heart disease is significantly higher. Ergo, it cannot be argued that there is a
causal correlation between fat consumption and deaths from heart disease. They need to be
other factors in play).
The logical fallacy
Yerushalmy and Hilleboe highlighted more errors:
1. 2. 3. the definitions of "heart disease" were arbitrary,
other nutrients (such as the animal protein) showed even stronger correlations,
and a greater share of carbohydrates in the diet was associated with more mortality
elevated for other causes.Their conclusion was clear: there was no evidence that fats caused the
heart disease.
Rather, the consumption of animal fat and protein seemed to reflect the level of development
cheap of countries: richer nations ate more fat and lived longer,
but they died more from chronic causes such as heart attack-not that fat was any
the cause.
In parallel with Yerushalmy and Hilleboe, the British physiologist also. John Yudkin observed
That heart disease seemed to be follow wellness, not fat.
Analyzing international data, Yudkin noted that countries with more income, more technology
and more comfort were also those with the higher coronary mortality.
He wrote with subtle irony:
"The strongest correlation I have found with coronary mortality is not with fat,
But with the number of radio and television licenses.
There is almost as good a correlation with the number of registered cars."
Behind Yudkin's humor was a powerful message:
heart disease could be A side effect of modern progress,
not butter or eggs.
In other words, what Keys interpreted as a "fat fault" could actually
reflect the price of development- sedentariness, stress, urbanization, food
industries and a radical change in lifestyle.
The forgotten side: carbohydrates and mortality
Yerushalmy and Hilleboe also deepened the relationship between fat, protein, and
carbohydrates and the causes of death other than heart disease.
The results were surprising:
- A higher percentage of calories from fat was associated with fewer deaths from
other causes (r = -0,657).
- Also the animal protein showed a negative relationship (r = -0.405).
- But the carbohydrates? Here the correlation was positive and strong: r = +0,671.
In practice, The higher the percentage of calories from carbohydrates, the more
increased mortality from causes other than heart disease.
But even here it is merely correlation, not causation.
- Yerushalmy and Hilleboe in 1957 were not proving that. carbohydrates
"cause" more deaths For other diseases.
- They were simply showing that, in the available data at the level of
populations, there was a positive relationship between percentage of calories from
carbohydrates and non-coronary mortality.This observation served to Questioning Keys' claim of certainty, not to
Reverse the blame.
When theory becomes dogma
Keys did not accept the criticism. In 1956 he launched the famous Seven Countries Study,
designed to prove his hypothesis.
The results?
- No correlation between total fats and heart disease.
- A correlation only with the saturated fats, but without proof of causation.
Nevertheless, the public narrative was consolidated: "saturated fat is bad for the heart."
And that belief, born of imperfect correlations and data selections, would drive
decades of guidelines, demonizing natural foods such as butter, eggs and meat.
The lecture
The origins of the myth about fats remind us of a fundamental principle:
a correlation is not a cause.
Keys never proved that saturated fat causes heart disease; yet his
assumption, amplified by the media and institutions, has shaped modern nutrition more than
any other theory.
As physiologist George Mann observed in the 1970s, "The diet-heart hypothesis is the most
great scientific deception of our time."
MORAL:
The science of nutrition is not static. Many of the dogmas we take today for
discounted arise from methodological errors and hasty generalizations. Understanding the history of the
fat also means learning to question what we think we know.
As always, I invite you to debate and discussion.
I look forward to seeing you in the comments...
See you soon and have a great weekend!
Oliver Ruatti

Thank you Oliver,
One question: if you are at cardiovascular risk , have carotid lacs, high cholesterolemia (LDLHigh) high blood pressure and already follow a healthy lifestyle: what dietary advice would you give?
Thank you!
Hi Oliver
I had been interested in visiting with your mom but unfortunately I was told she no longer receives....
I have an autoimmune condition I did paleo keto carnivore and lions but from blood tests nothing changed...I also did water fasting 7 days twice....
Pathology is hemolytic anemia by cold agglutinins.
It's a rash -- sorry to bother you.
Thank you for the simple and complete explanation
I have suffered from hypercholesterolemia for as long as I can remember (I am 56 years old) ...since the maximum total cholesterol values were 250 mg. I to date,without Ezetimibe I am at 360
I recently have other parameters LDL HDL etc. checked ...
They made me 'swallow' soybean oil and margarine for years.
Since following the newly acquired directions I have definitely improved my digestion and the low-grade inflammation that is so much talked about. Slowly I have implemented many changes from intermittent fasting to congruent protein consumption (including eggs!) ,from earthing in the garden in the morning to cold shower and photo I modulation.
The trouble is that often the people I talk to about these things are obtuse,unwilling to change. Practically....a rubber wall. Curiosity is the engine that drives us to knowledge and it is not such a widespread endowment!
Unfortunately, it is not easy to find professionals who have this open mindedness. I live in Genoa and often have to move around looking for doctors I can trust.
Thank you again for your efforts.
Thank goodness there are people and future doctors who give us some hope...!!!
Good work
Illuminating article. I plan to reread it several times to fix the principles set forth.
Doctor I am more and more convinced that I did the best thing by following your advice. Thank you .
Thank you very much as always for the comprehensive and clear explanation of all this data. I have been following the low carb diet for a year now and I must say that I am doing very well. The only thing I cannot help but wonder is how is it possible that an entire scientific community did not catch all these discrepancies and omissions. I can imagine that at some point the pharmaceutical companies had an influence on guidelines, etc. but I wonder how it could have gotten to that point. Did no one other than the scientists mentioned question whether the theory was wrong? No polemical intent, just a doubt I have whenever some acquaintance questions the way I eat. Thank you very much
Thank you Dr. Tomas for what you do in disseminating truths that many
They do not know and do not elaborate One of his followers
Hi Oliver, Thank you thank you thank you, we finally put a name to this myth! When I say that I eat about 30-40 eggs a week, meat and butter to my heart's content, I am looked at with wide eyes. All the more so because I am a nurse and should know very well that fat raises cholesterol! But the thing that discourages me most is that even the new generation medical class is convinced of this! I was even told by one of them, "If you eat all these eggs you will get gout"😝! But I go on my way and try to spread the truth about cholesterol to people who are willing to understand! Every once in a while I find someone! Thank you, your mother and people like you for your efforts...don't give up!
Good morning Doctor..my son checked, cholesterol 300 and triglycerides 600 I am very worried .. prescription of rosuvastatin and omega 3 and elimination of some foods..what do you think of the prescribed treatment..thank you
But then what raises cholesterol? And especially what causes plaques in the arteries? Especially soft plaques, the most dangerous ones? How to do prevention?
Hi Anna, wonderful question, because this is where one of the biggest misunderstandings of modern medicine lies. Cholesterol per se is not the culprit, but rather the "witness" to a deeper process involving inflammation, oxidation and vascular damage.
High cholesterol per se does not "ruin" arteries. On the contrary, cholesterol is a repair molecule: it is sent into tissues, including blood vessels, when there is damage to repair. So a high value can often reflect a defense mechanism, not disease. However, when the internal environment is inflamed or oxidized, cholesterol-carrying LDL particles can change and become dangerous.
So what really raises cholesterol? In many cases, it is not the amount of fat you eat, but rather the factors that push the liver to produce more of it or that hinder its proper recycling. Here are the main ones:
- Excess sugar and refined carbohydrates, which stimulate insulin and increase the production of triglycerides and VLDL in the liver.
- Chronic inflammation (due to stress, smoking, latent infections, poor sleep).
- Thyroid dysfunction or slowed metabolism.
- Oxidative stress from excess free radicals and deficiency of natural antioxidants (vitamin E, C, CoQ10).
- Carbohydrates and industrial fats together (sweets, snacks, margarines, refined vegetable oils): the most dangerous combination.
All these factors can not only increase circulating cholesterol, but more importantly create the conditions that lead to plaque formation.
Atherosclerotic plaques do not come out of nowhere. They begin with minor damage to the endothelium, the inner layer of the arteries. This damage can result from glycation (high sugars), hypertension, toxins, or oxidative stress. When the endothelium becomes damaged, LDL stops there to "repair the wall." However, if these LDLs are oxidized or inflamed, they are recognized as abnormal by the immune system and engulfed by macrophage cells that become "foam cells." This is how plaque is formed.
The soft plaques, which are the most dangerous because they can rupture and cause thrombi, are precisely those that are richest in oxidized and inflamed lipids. They are not the "fat plaques" as people think, but active inflammatory lesions.
This means that prevention is not done by lowering cholesterol, but by turning off the inflammation and oxidation that damage it.
Prevention, therefore, means:
- Keep blood sugar stable and reduce insulin (by eliminating sugars and flours);
- Avoid refined vegetable oils and oxidized industrial products;
- Increase intake of natural fats and antioxidants (butter, egg yolks, fish, olive oil, quality meat and offal);
- Maintain good thyroid function and an active metabolism;
- Exposure to sunlight, good sleep, managing chronic stress;
- and, if necessary, check real risk markers such as ApoB, LDL-P, Lp(a), ultrasensitive PCR(inflammation) and fasting insulin.
Oliver
Perfect. But everyone says anyway cholesterol over 300 should be decreased, what should be done?
Is it enough to remove carbs and sugars?
And after about how long can we eventually see results?
Thank you
Hi Maria, this is a very important question, and the truth is that the number "300" alone is not enough to decide whether cholesterol is a problem or not. You always have to understand what kind of cholesterol is elevated, in what context, and why.
Total cholesterol (e.g., 277 or 300) is the sum of HDL, LDL and a small portion of VLDL. But if, as in your case, HDL is high (77) and triglycerides are low, this indicates a healthy, well-regulated lipid metabolism, not a risk. In these situations, total cholesterol is high only because HDL and LDL are both high and well-functioning, not oxidized.
It is not the absolute number of LDL (195, 200 or 220) that makes the difference, but the quality of the LDL particles. There are small, dense LDLs, which are easily oxidized and can penetrate the endothelium increasing cardiovascular risk, and there are large, "floating" LDLs, which are much less oxidizable and generally harmless. Diets high in sugar and refined carbohydrates promote small, dense LDL, while low-carbohydrate or carnivorous diets increase large, physiological LDL.
Reducing sugar and starches is always a good idea: it lowers triglycerides, reduces inflammation and LDL oxidation, increases HDL, and improves insulin sensitivity. However, if you reduce carbohydrates too abruptly and increase fat (especially saturated fat) too much, cholesterol may rise temporarily in the first few months. This is not because there is a real risk, but because the liver is adjusting to the new metabolism. After 3-6 months, the lipid profile tends to stabilize and improve markedly.
Already after 4-6 weeks of a diet with reduced sugars and natural fats (eggs, meat, fish, butter, olive oil), triglycerides decrease and HDL increases. LDL stabilizes within 3-6 months. Total cholesterol may remain high, but what really matters are other more accurate indicators such as the triglyceride/HDL ratio and, most importantly, ApoB or total LDL particle number (LDL-P), which you can ask to be measured if you want to assess risk more accurately.
To sum up: you don't need to "lower" cholesterol, you need to improve its context. Cut out refined sugars, flours and vegetable oils. Eat real foods, rich in natural fats and quality proteins. Get moving, get good sleep and reduce chronic stress. The liver alone will do the rest, and in a few weeks your lipid profile will change for the better.
A high number is not a condemnation, but a message from the body, "I'm using fat as fuel." What really matters is not how much cholesterol you have, but what metabolic state your body is in.
Oliver
Thank you for the very precise explanation
In fact I was a little worried because I have been following anti-inflammatory for 2 months and the results of the blood test a few days ago gave me raised values of total cholesterol from 216 to 336 and I was worried but then I noticed that the triglycerides were lowered and HDL was raised And at this point I am overjoyed that I can continue (despite what the doctor will surely tell me) the diet I am doing and that I am fully satisfied with and I will redo the tests in the spring x see if everything has stabilized
Thank you very much for making me aware of the needs of my body to be well
Very good analysis...I am personally convinced.
"Knowledge makes man free "
Thanks Oliver, see you next time, I hope!!!
Dearest Dr. Cristina, thank you from the bottom of my heart for the information you give us! Regarding cholesterol, it is a topic dear to me, having high values (cholesterol 277 - Hdl 77 - Ldl 195). I have been following the various studies with much interest. Now I am left with a question: who produces the "bad" cholesterol? I don't know if it will be possible to get a simple answer, but I hope so! Again Thank you and have a good Sunday!
Ornella Giuliani
Hi Ornella thank you for your message.
In fact, no one "produces" bad cholesterol, because cholesterol is not bad per se.
All the cholesterol in the blood is produced by our own body, mainly by the liver (about 80%), and only a small part comes from food.
The term "bad cholesterol" refers not to the cholesterol itself, but to the type of particle that carries it in the blood:
Lipoprotein type:
- LDL (low-density lipoprotein): carries cholesterol from the liver to the tissues. Referred to as "bad cholesterol"
- HDL (high-density lipoprotein): carries cholesterol from tissues to the liver. Referred to as "good cholesterol"
How LDL ("bad") is formed.
1. The liver produces VLDL (very low-density lipoprotein), which transports triglycerides and cholesterol to tissues.
2. Tissue cells remove triglycerides from these particles → what remains becomes LDL.
LDL is used to distribute cholesterol where it is needed (cell membranes, hormones, vitamin D .
4. Only if LDL stays in the bloodstream too long and becomes oxidized or inflamed does it become potentially dangerous to the arteries.
So it is the inflammatory or oxidative metabolic environment that transforms normal LDL into harmful forms.
Some factors that can promote this transformation are:
- High blood sugar and insulin resistance
- Oxidative stress (smoking, antioxidant deficiencies, etc.)
- chronic inflammation
- sedentariness
- Excess refined carbohydrates or oxidized vegetable oils
All cholesterol is "good": it is used to build hormones, membranes and vitamin D. LDL is like a courier/shuttle, carrying cholesterol to tissues that require it. Without it: the endocrine glands, nervous system, skin, cell membranes, immune cells and so on could not generate and regenerate, maintain stability and function properly.
But if the metabolism is inflamed or oxidized, LDL particles can become damaged and become "bad."
Basically: there is no such thing as bad cholesterol-there are bad conditions.
Oliver
Thank you for the critical re-reading of the scientific literature, which many people cannot access. I find the insights very interesting, and I confess that many nutrition and health specialists (I'm thinking of nutritionists and cardiologists) know nothing about it.
I, since I have given the green light to animal protein (eggs and meat) have defeated reflux and regained my energy.
Hi Oliver and thank you for your insightful analysis!
I fully agree with everything you analyzed, the only problem is getting people (who still don't know) to understand this. Unfortunately they take the doctor's word for fool's gold and having only doctors who still rely on the guidelines ,you understand that it is very hard to spread these beliefs, because all they do is say that cholesterol is dangerous and needs to be lowered. Thank you for your continued knowledge, keep it up!
I don't know what to do or who to believe anymore..col. total 434 - HDL 92 - Triglycerides 73 - LDL oxidized to 282 - LDL 330. I think I am a LHMR person, thin and I exercise..In your opinion is it to take Nilemdo and Ezetimibe?I did coronary CT and Tsa and everything is clean..Thanks if you can answer me..